New Research Shows RHC Program Continues to Grow
Sarah Hohman, Director of Government Affairs
The National Center for the Analysis of Healthcare Data (NCAHD), working together with the NARHC Research and Education Foundation (REF), recently completed research on the market health of the Rural Health Clinics (RHC) program. This research was designed to give policymakers and the rural health community a more detailed picture of trends occurring in the RHC program across the United States. You can find the full NCAHD research and methodology report here.
The research evaluated federal RHC data housed by the Center for Medicare and Medicaid’s (CMS) Quality, Certification, and Oversight Reports (QCOR) between 2020-2022, and revealed four key trends in the RHC landscape:
1-The RHC program continues to grow;
2-For the first time in likely decades, there were more new independent RHCs than new provider-based RHCs in 2022;
3-RHC “terminations” remained largely consistent in the 2020-2022 period with a slight uptick in total closures in 2022; and
4-Of the RHCs that are listed as terminated in the federal data, 47% are providing care through a different model, 33% of terminated RHCs have truly closed with no healthcare being provided at that location, and roughly 19% are still operating as an RHC, just under a new CMS Certification Number (CCN).
1-Overall Growth of RHC Program
In the three-year period between 2020 and 2022, 997 new RHCs opened and 330 RHCs terminated (details on the “terminated” status can be seen below). The RHC program has seen consistent growth for decades and the 2020-2022 period was no different (See Table 1).
NCAHD conducted research into each of the 330 RHCs that were listed as terminated in the QCOR database and refined the data further into the following categories:
1-CCN Change – Describes an entity that is still operating as an RHC but underwent a change in ownership that resulted in a new certification number.
2-Closed – Describes an RHC that terminated their RHC status, and no healthcare is being provided at that address.
3-No Longer Participating – Describes RHCs that terminated their RHC status and are no longer participating in Medicare as RHCs but are still providing care under some other model/facility type.
| RHC Changes | ||||
| New | CCN Change | Closed | No Longer Participating | |
| 2020 | 345 | 42 | 35 | 47 |
| 2021 | 350 | 12 | 35 | 47 |
| 2022 | 302 | 10 | 40 | 62 |
| Total | 997 | 64 | 110 | 156 |
Table 1-Total RHC Changes (2020-2022)
2-New Independent RHCs Overtook New Provider-Based RHCs in 2022
For the first time in likely decades, new independent RHC development outpaced new provider-based RHC development (See Figure 1). Given the major reforms to Medicare RHC reimbursement that occurred at the end of 2020, this trend is not surprising but nonetheless notable. Despite the name, freestanding or “independent” RHCs can in fact be owned by hospitals or health systems, so this fact does not necessarily mean that hospital/clinic consolidation has slowed in the RHC space. The current benefits of opening new provider-based RHCs are mostly related to 340B participation given that as of 2021, new provider-based RHCs are treated the same as new freestanding RHCs in terms of Medicare reimbursement policy.
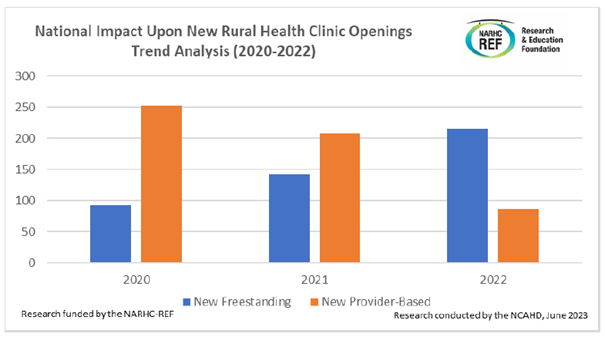
Figure 1-National Impact of New RHCs (2020-2022)
3-RHC Terminations Remained Largely Consistent with a Slight Increase in Terminations in 2022
From 2020 to 2022 there was not a major spike in the number of RHCs leaving the program. Concern that there would be an exodus of RHCs leaving for other models due to the Medicare payment reforms has not, at this point, manifested in the data (See Table 2).
In fact, the slight increase in terminations in 2022 is actually attributable to a slight increase in the number of freestanding RHCs closing or converting to other models, not provider-based RHCs.

Table 2-RHC Changes by Ownership Type
4-Only 33% of RHC Terminations Represent True Closures
NCAHD research showed that in approximately two-thirds of the “terminated” RHC cases there was still healthcare being provided at that address. The federal data marks these all as “terminated” RHCs, but in 19% of these cases there is still an RHC operating at that address, just under a different CCN. Furthermore, while NARHC would certainly want RHCs to be the model of choice for rural, medically underserved communities, the most important thing is that these communities have access to care. Thankfully, this data shows that nearly half (47%) of the RHCs that “terminated” actually remained open under a different healthcare delivery model such as fee-for-service or the community health center model.
Nevertheless between 2020 and 2022, in 110 (55 freestanding and 55 provider-based) cases, the RHC did close, and as of April 2023 when this data was gathered, there was no healthcare being provided at that specific address. Further research would be necessary to analyze how community-wide access to outpatient care was impacted by these closed RHCs.
The NARHC Research and Education Foundation was established in 2021 to establish a repository of RHC relevant research and analysis that can be available for use by anyone interested in the success of the RHC program. REF supported research will support and guide NARHC’s ongoing policy efforts.
Please contact Nathan Baugh, NARHC Executive Director or Sarah Hohman, Director of Government Affairs at Nathan.Baugh@narhc.org or Sarah.Hohman@narhc.org with any questions.
